
Anterior Cruciate Ligament Reconstruction
What is ACL Reconstruction?
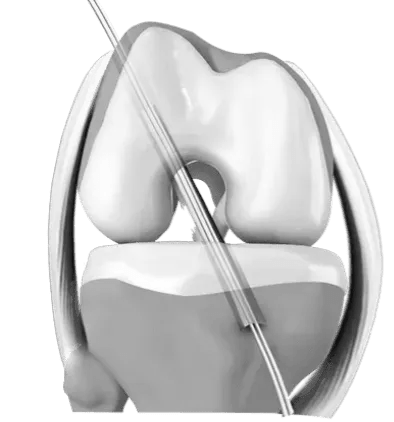
The Anterior Cruciate Ligament is one of the major stabilising ligaments in the knee. It is a strong rope-like structure located in the centre of the knee running from the femur to the tibia.
When this ligament tears unfortunately it doesn’t heal and often leads to the feeling of instability in the knee.
ACL reconstruction is a commonly performed surgical procedure and with recent advances in arthroscopic surgery can now be performed with minimal incisions and low complication rates.
What Does the ACL Do?
The ACL prevents the tibia (shin bone) moving abnormally on the femur (thigh bone). When this abnormal knee movement occurs, it is referred to as knee instability and the patient is aware of this abnormal movement.
Often, other structures such as the meniscus, the articular cartilage (lining the joint) or other ligaments can also be damaged at the same time as a cruciate injury and these may need to be addressed at the time of surgery.
- Most injuries are sports-related involving a twisting injury to the knee.
- It can occur with a sudden change of direction, a direct blow, e.g., a tackle, landing awkwardly.
- Often there is a popping sound when the ligament ruptures.
- Swelling usually occurs within hours.
- There is often the feeling of the knee popping out of the joint.
- It is rare to be able to continue playing sports with the initial injury.
What are the Symptoms of ACL Tears?
Once the initial injury settles down, the main symptom is instability or giving way of the knee. This usually occurs with running activities but can occur with simple walking or other activities of daily living.
What are Treatment Options for an ACL Tear?
Initial
Initial management post-injury includes:
- Rest
- Ice
- Elevation
- Bandage
After the initial period of rest, it is often recommended to start exercises with a physiotherapist. The goal is to regain your range of motion, reduce the swelling in the knee and make the thigh muscles strong again.
Long Term
Not everyone needs surgery. Some people can compensate for the injured ligament with strengthening exercises or a brace.
It is strongly advised to give up sports involving twisting activities if you have an ACL injury. Episodes of instability can cause further damage to important structures within the knee that may result in early arthritis.
What are the Indications for ACL Surgery?
Suitable candidates for ACL Reconstruction Surgery include:
- Young patients wishing to maintain an active lifestyle.
- Sports involving twisting activities, e.g., soccer, netball, football
- Giving way with activities of daily living.
- Physically demanding occupations, e.g., policemen, firemen, roofers, scaffolders.
It is advisable to have physiotherapy prior to surgery to regain motion and strengthen the muscles as much as possible.
Who Should Consider ACL Reconstruction?
The indications for undergoing an ACL reconstruction are
- Recurrent symptoms of ACL instability following an ACL rupture
- A high likelihood of developing ACL instability due to a combination
- Age
- Activity level
- Activity type
A knee that has an ACL Rupture and a Meniscal Tear often combine with improved outcomes.
ACL Reconstruction vs ACL Repair
Repair involves keeping the original ligament by directly suturing the two ends of the rupture together. Attempts at repair of ACL tears are now largely historical due to the high rate of failure of the surgery.
All ACL surgery nowadays is a reconstruction. This involves replacing the damaged tissue with a substitute tissue called a graft. The most commonly used grafts involve use of tissue from the patient (autografts). Tissue from donor patients (allografts) can also be used, as can synthetic ligaments.
ACL Reconstruction Procedure
Surgery is performed as a day procedure or an overnight stay.
The surgery usually takes between 60–90 minutes
Surgical techniques have improved significantly over the last decade, complications are reduced and recovery much quicker than in the past.
The surgery is performed arthroscopically.
- The ruptured ligament is removed and then tunnels (holes) in the bone are drilled to accept the new graft.
- This graft which replaces your old ACL is most often the hamstring tendon, patella tendon or quadriceps tendon.
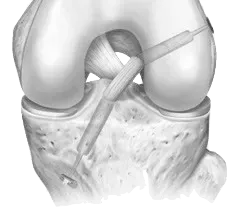
- The graft is prepared to take the form of a new tendon and passed through the drill holes in the bone.
- The new tendon is then fixed into the bone with various devices to hold it in place, while the ligament heals into the bone (usually 9-12 months).
- The rest of the knee can be clearly visualized at the same time and any other damage is dealt with, e.g meniscal tears.
- The wounds are then closed and a dressing applied.
What do the Post-operative Steps Include?
Pain Management
You will have pain medication by tablet or in a drip (intravenous). A splint is sometimes used for comfort.
Wound Care
Leave any waterproof dressings on your knee until your post-op review.
- You can put all your weight on your leg.
- Put ice on the knee for 20 minutes at a time, as frequently as possible.
Post-op review
The first review will usually be after 10-14 days.
Physiotherapy
You will be seen by a Physiotherapist who will teach you to use crutches and show you some simple exercises to do at home.
Exercise and therapy can begin after a few days or can be arranged at your first post-op visit.
Complications
If you have any redness around the wound or increasing pain in the knee or you have a temperature or feel unwell, you should contact our office or your GP as soon as possible.
Why is Rehabilitation for ACL Reconstruction Essential?
Physiotherapy is an integral part of the treatment and is recommended to start as early as possible. Pre-operative physiotherapy is helpful to better prepare the knee for surgery. The early aim is to regain range of motion, reduce swelling and achieve full weight-bearing.
The remaining rehabilitation will be supervised by a Physiotherapist and will involve activities such as exercise bike riding, swimming, proprioceptive exercises and muscle strengthening. The rehabilitation program is based on achievements rather than time frames. Your physiotherapist will determine when you are ready for the next step.
Please refer to the postoperative download section for the full rehabilitation program.
ACL Reconstruction Rehabilitation Program
Each step of the rehab program is based on achievements. Only after you can safely perform the exercises in each stage, you will progress to the next stage. Below is an overview of the stages with rough time frames. Keep in mind, these time frames are indications only and may not apply to your specific rehabilitation program.
What are the Risks & Complications of ACL Reconstruction?
Complications are not common but can occur. Prior to making the decision to have this operation, it is important you understand these so you can make an informed decision on the advantages and disadvantages of surgery.
These can be medical (Anaesthetic) complications or surgical complications including: bleeding, infection, blood clots, stiffness, pain, numbness, swelling, re-rupture.
Summary
Anterior Cruciate Ligament reconstruction is a common and very successful procedure. It is generally recommended in the patient wishing to return to an active lifestyle, especially those wishing to play sports involving running and twisting.
The above information hopefully has educated you on the choices available to you. If you have any further questions you should consult our staff.



